
Semaglutide (aka, Ozempic/Wegovy), reduces the risk of cardiovascular disease, even if you don’t have diabetes. But we still have a lot to learn.
A new paper published last week in the New England Journal of Medicine reported very interesting results from a clinical trial of semaglutide, the active ingredient in both Ozempic and Wegovy.
The trial was one of the first to look at clinical outcomes for people who are overweight or obese but do not have diabetes, the condition the drugs were first designed for.
The large trial included 17, 604 people who were randomized to either one weekly injection of 2.4 mg of semaglutide or a placebo. The participants were all 45 years of age or older and had pre-existing cardiovascular disease, but not diabetes. The participants received the treatment and were followed up to look for disease for close to 3 years.
Those who received semaglutide had a 20% lower relative risk of any cardiovascular event happening over those 3 years (death, non-fatal heart attack, non-fatal stroke). In absolute terms, a CVD event occurred in 8% of the placebo group compared to 6.5% of the treatment group over this time frame. Is this a lot? Given that heart disease is the leading cause of death in the US, killing almost 700,000 people per year, a 20% reduction in risk is pretty significant and on par with the estimated benefit of statins. These benefits also grew over time during the study, so it’s possible the benefits could be even larger beyond three years.
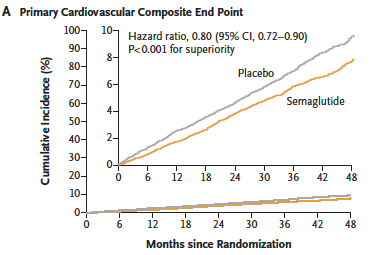
Source: Lincoff, A. Michael, et al. “Semaglutide and cardiovascular outcomes in obesity without diabetes.” New England Journal of Medicine (2023).
Besides the “primary” endpoints of death, heart attack, and stroke, the study also examined “secondary” outcomes such as how much the drug lowered blood levels of known risk factors for heart disease. I found these results particularly striking. Levels of C-reactive protein (CRP), a marker of inflammation that is predictive of heart disease, dropped by almost 38% in the semaglutide group. Triglycerides, a type of fat that circulates in the blood, dropped by almost 16%. Fewer patients on the treatment who were in the pre-diabetes blood glucose range progressed to diabetes over this time period as well. It’s notable that most of these patients were already taking cholesterol or blood pressure medications, meaning these improvements were above and beyond the protective effects of those other drugs.

As a mortality researcher who knows too well how deaths from cardiovascular disease are wreaking havoc on life expectancy trends in the US, I have to admit the trial results coming out about semaglutide (and other drugs in the class of GLP-1 agonists) have me pretty excited.
It’s still very early days, and there is much more we need to learn about the potential downsides and unforeseen long term effects of these drugs. Read our recent post for example about potential impacts of these drugs on the effectiveness of contraception, something that definitely needs more study. In this recent clinical study of over 3 years, serious adverse events were actually more common in the placebo compared to the treatment group. This suggests that at least in people who are at high risk for diabetes and cardiovascular disease, potential benefits likely outweigh the risks. However, more participants taking semaglutide discontinued the treatment compared to placebo due to minor adverse events such as gastrointestinal discomfort such as nausea and diarrhea, which is an obvious downside. It’s likely that people would need to keep taking the drugs to see these benefits, as is the case with other medications for diabetes and cardiovascular disease.
Semaglutide has already been shown to dramatically reduce blood glucose and diabetes risk in previous clinical trials, and these new results are showing that it might have broader benefits. As we all know from the news (and TikTok), these drugs also induce significant weight loss (10-15% of body weight depending on the trial). The drugs impact diabetes through their impact on insulin and glucose regulation, but they also slow the emptying of the stomach and make people feel full longer, reducing overall food consumption.
A staggering 42% of people in the US are classified as obese up from 15% in 1980, and the growth in obesity prevalence in the US is accelerating rather than slowing. This phenomenon is happening globally as well, although the US led the charge. The obesity epidemic is a complex social problem rooted in changing technology and economic development. While our genetics and individual will-power have not changed dramatically in the last 40 years, our food and physical environments definitely have. This means that while the diet industry focuses intensively on individual lifestyle choices, the deck is clearly stacked against most people for maintaining a healthy weight in modern environments. There is currently no example of a society that has reversed the course of its obesity epidemic.

Figure: Age-adjusted trends in overweight, obesity, and severe obesity among men and women aged 20–74: United States, 1960–1962 through 2017–2018, CDC
It’s also very difficult for people who are already obese to sustain significant weight loss, as the body fights very hard to retain fat through its regulatory processes. Up until now, bariatric surgery, a very invasive surgical procedure, has been the only intervention to demonstrate good success in sustained weight loss. This does not mean that lifestyle changes are not beneficial – exercise has tons of health benefits in its own right, as does eating better food. And lifestyle changes can help prevent further weight gain, which is really important as we age. So while we should continue to educate people about healthier lifestyles AND address the bigger picture “structural” causes of obesity like our food industries, it’s clear that we also need all the additional help we can get.
For me, the development of semaglutide and other GLP-1 agonists feels like the possibility of something potentially really huge for population health. (For an interesting read on the scientific origins of this breakthrough and the woman who had to fight for her contributions to be recognized, read here). There are also many similar drugs currently in development (including oral preparations rather than injections), so it’s very likely that the quality of these drugs will get better and the price will come down. So while there is a long road ahead with plenty of potential land mines along the way, this health researcher is cautiously optimistic about the promise of these new tools to help our metabolic and cardiovascular health.
Stay safe, stay well. Stay tuned for more breaking research.

